 手术jones骨折第5跖骨基底骨折切开复位内固定术.docx
手术jones骨折第5跖骨基底骨折切开复位内固定术.docx
- 文档编号:11708834
- 上传时间:2023-03-30
- 格式:DOCX
- 页数:12
- 大小:414.89KB
手术jones骨折第5跖骨基底骨折切开复位内固定术.docx
《手术jones骨折第5跖骨基底骨折切开复位内固定术.docx》由会员分享,可在线阅读,更多相关《手术jones骨折第5跖骨基底骨折切开复位内固定术.docx(12页珍藏版)》请在冰豆网上搜索。
手术jones骨折第5跖骨基底骨折切开复位内固定术
Jonesmann骨折指第五跖干骺端与骨干连接部骨折。
英国骨科医生Sir Robert Jones(1857–1933)自己跳舞后发生此类骨折并首先描述,故此得名。
Jonesfracturesoccurinasmallareaofthefifthmetatarsalthat receiveslessblood andisthereforemorepronetodifficultiesinhealing.AJonesfracturecanbeeitherastressfracture(atinyhairlinebreakthatoccursovertime)oranacute(sudden)break.Jonesfracturesarecausedbyoveruse,repetitivestress,ortrauma.Theyarelesscommonandmoredifficulttotreatthanavulsionfractures.
A Jonesfracture isa fracture ofthe diaphysis ofthe fifthmetatarsal ofthe foot.Thefifthmetatarsalisatthebaseofthesmall toe.The proximalend,wheretheJonesfractureoccurs,isinthemidportionofthefoot.PatientswhosustainaJonesfracturehave pain overthisarea,swelling,anddifficultywalking.Thefracturewasfirstdescribedby British orthopedicsurgeonSir RobertJones,whosustainedthisinjuryhimselfwhiledancing,inthe AnnalsofSurgery in1902.
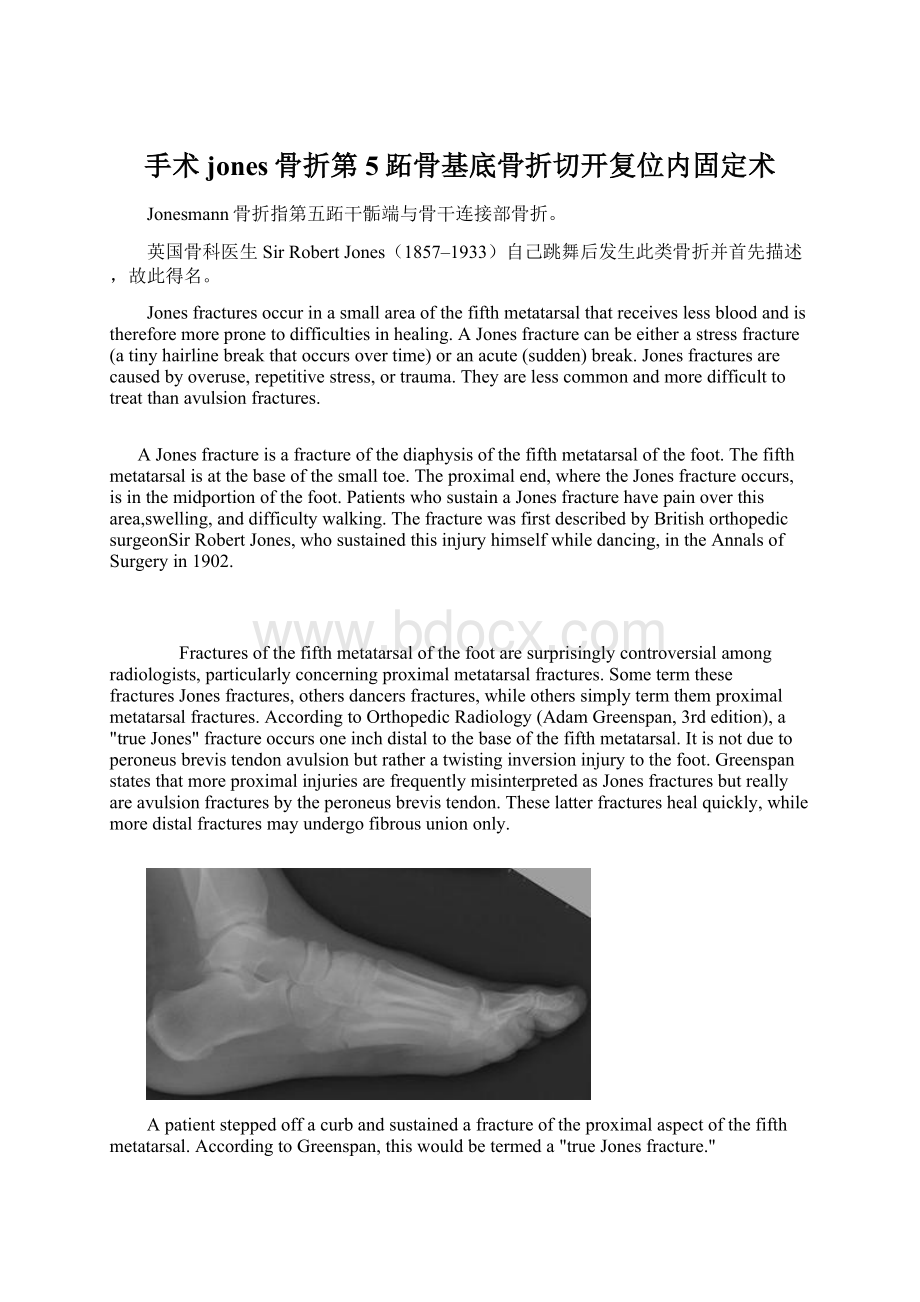
Fracturesofthefifthmetatarsalofthefootaresurprisinglycontroversialamongradiologists,particularlyconcerningproximalmetatarsalfractures.Sometermthesefractures Jonesfractures,others dancersfractures,whileotherssimplytermthem proximalmetatarsalfractures.AccordingtoOrthopedicRadiology(AdamGreenspan,3rdedition),a"trueJones"fractureoccursoneinchdistaltothebaseofthefifthmetatarsal.Itis notduetoperoneusbrevistendonavulsionbutratheratwistinginversioninjurytothefoot.GreenspanstatesthatmoreproximalinjuriesarefrequentlymisinterpretedasJonesfracturesbutreallyareavulsionfracturesbytheperoneusbrevistendon.Theselatterfractureshealquickly,whilemoredistalfracturesmayundergofibrousuniononly.
Apatientsteppedoffacurbandsustainedafractureoftheproximalaspectofthefifthmetatarsal.AccordingtoGreenspan,thiswouldbetermeda"trueJonesfracture."
Incontradistinction,thispatientsustainedafractureoftheproximalaspectofthefifthmetatarsal.Greenspantermsthisanavulsioninjury.Inanavulsionfracture,asmallpieceofboneispulledoffthemainportionofthebonebyatendonorligament.Thistypeoffractureistheresultofaninjuryinwhichtheanklerolls.Avulsionfracturesareoftenoverlookedwhentheyoccurwithananklesprain.
Treatment:
IfaJonesfractureisnotsignificantlydisplaced,itcanbetreatedwitha cast,splintorwalkingbootforfourtoeightweeks.Patientsshouldnotplaceweightonthefootuntilinstructedbytheirdoctor.Three-fourthsoffracturestreatedlikethisshouldheal.
Inthecaseofacutefractureinanathlete,adynamiccompressionplatecanbeplacedonthetensionsideofthefracture,K-WirewithMonofiamentwireinafigure8fashionduetothenatureofatransversefracture.Internalfixationwithcorticalorcancellousscrewwouldrequireanobliquefracturethatcouldbeaddressedthrough"Theruleof2's"inregardstoInternalfixationwithscrews.
Othertreatmentscommonlyencouragedareincreasedintakeof vitaminD and calcium.
Thisinjurymustbedifferentiatedfromthephysiologicdevelopmental apophysis commonlyandnormallyoccurringatthissiteinadolescents.Differentiationispossiblebycharacteristicssuchasabsenceofsclerosisofthefracturededges(inacutecases)andorientationofthelucentline:
transverse(at90degrees)tothemetatarsalaxisforthefracture(duetoavulsionpullbytheperoneusbrevismuscleinsertingattheproximaltip)-andparalleltothemetatarsalaxisinthecaseoftheapophysis.
Jonesfracturescanbecomechronicconditionsifthefracturefailstounite,orheal.Ifthisisthecase,surgerywilllikelyberecommendedtosecurethefractureinplacewithascrew,andbonegraftmaybeusedtostimuateahealingresponse.
-SurgicalTreatment:
(JonesFrx);
-patientispositioninpartiallateralpositiononbeanbag;
- flouroscopy:
-underflourscopicguidence,aKwireisinsertedfordeterminationofproperpositionandlength;
- mostcommonmistakeistodirectthedrillplantarly,ratherthanparallelw/theshaftofmetatarsal;
- secondmistakeistoopositiontheguidewireusingtheobliqueview;
-notethatthemetatarsalshaftismorenarrowontheAPview,anditis possibleforthepintobecenteredontheobliqueview
whereasonAPviewthepiniseccentricallypositioned;
- incision:
-longitudinalincisionismadeoverdistalmetatarsal;
-takecaretoavoidbranchesofthesuralnervewhichcancoursedorsally,andlaterallyovermetatarsal;
-peroneusbrevisisretractedinferiorly;
- insertionofthistendonmayobscuretheproperdrillentrysite;
- localbonegraft:
-canbeobtainedfromtuberosityandfrombonebitsfromthedrill;
- implants:
-considerinsertionof 4.5cancellousbonescrews, 4.5mmcannulatedscrews(whichareusedinmostcases)buthave available5.5cannulated(and solid) screwsand6.5mmcannulatedscrews;
-diametershoulddependonwidthofthecanal(letthescrewtaphelpdeterminethebestsize);
-ineithercase,threadsmustcrossthefrxline;
-lengthisusuallybetween40-55mm;
-considercountersinkingthescrewtoavoidprominenceofthescrewhead;
-in reportbyIPKelly, authorsnotedthatfailureismorelikelywhensmallerdiameterscrews areused;
-experimentalJonesfractureswerecreatedin23pairsofhumancadaverfifthmetatarsals,whichwerefixedusingeither5.0mmor6.5mmscrews;
-frxstiffnessandpull-outstrengthsweremeasuredforeitherscrewtypeand relationshipswithbone densityand canaldiameterweredetermined;
-poorthreadpurchasewithinthemedullarycanalwasnotedwiththe5.0mmscrews,whileexcellentpurchasewasnotedwith6.5mmscrews;
-pull-outstrengthtestingrevealedsignificantlyhigherpulloutstrengthsforthelarger6.5mmscrews;
-theauthorsconcludethatlargerdiameterscrewsmaybemoreappropriateforintramedullaryscrewfixationofJonesfractures;
-ref:
TreatmentofJonesFractureNonunionsandRefracturesintheEliteAthleteOutcomesofIMScrewFixationWithBoneGrafting
- postop:
patientswill requireprotectedpostoperative wtbearing;
1、解剖方面考虑:
恢复跖骨头的队列关系是非常重要的前足的力学目标:
如下图示:
在正位,应是“顺流而下”的表现,且与对侧足对称,这是恢复正常跖骨长度的保证。
另一个需要恢复的重要结构是跖骨水平线,需保持其均在一个水平线上。
需要注意的是,在第一跖骨,是籽骨在承重,而不是第一跖骨头,因此,序列对应关系应与籽骨为准。
任何力线改变均可引起站立相和推离相时疼痛及胼胝形成。
2、螺钉或钢板固定:
固定这种骨折,因尽可能使其稳定。
横行骨折线时,单独拉力螺钉固定即可。
3、手术入路:
详见后。
4、复位:
骨折在直视下复位,因为其为横形骨折,复位满意后用复位钳保持复位。
5、拧入螺钉:
从腓骨短肌肌腱止点处,稍向内侧倾斜方向打入导针,这样可以抓住远骨折端的内侧骨皮质,增加稳定。
骨折近端应做成滑动孔,以允许骨折块间加压,螺钉直径应根据骨情况来选择,常选用3.5或4.0mm螺钉固定。
6、另一种固定方式:
髓内螺钉固定:
选髓内螺钉固定,螺钉直径要与髓腔匹配,螺钉必须有充足直径以获得稳定加压固定,根据髓腔的大小,可选用3.5或4.5mm皮质螺钉固定,在体型高大患者,可能需用6.5mm松质骨螺钉固定。
1、注意保护血运:
避免广泛深度暴露、过度牵拉;多个跖骨骨折应采用单独切口,避免增加软组织损伤;在足部保护静脉回流是非常重要的。
2、解剖:
小隐静脉位于切口部位的皮下;在静脉的深面是小趾外展肌;腓肠神经(与小隐静脉伴行)的分支应给予保护。
3、皮肤切口:
切口开始于可触及的第5跖骨茎突处,依据需要向远端延伸。
切口要位于足部掌侧皮肤与背侧皮肤的交界处。
4、深层分离:
显露第5小趾外展肌筋膜,并纵向切开。
5、骨质显露:
使用拉钩,向背侧牵开皮肤及背侧筋膜,向掌侧牵开肌肉,显露第5跖骨基底。


- 配套讲稿:
如PPT文件的首页显示word图标,表示该PPT已包含配套word讲稿。双击word图标可打开word文档。
- 特殊限制:
部分文档作品中含有的国旗、国徽等图片,仅作为作品整体效果示例展示,禁止商用。设计者仅对作品中独创性部分享有著作权。
- 关 键 词:
- 手术 jones 骨折 跖骨 基底 切开 复位 固定
 冰豆网所有资源均是用户自行上传分享,仅供网友学习交流,未经上传用户书面授权,请勿作他用。
冰豆网所有资源均是用户自行上传分享,仅供网友学习交流,未经上传用户书面授权,请勿作他用。
 铝散热器项目年度预算报告.docx
铝散热器项目年度预算报告.docx
-
牛津上海版通用小学英语三年级上册Unit 12同步练习2II 卷.docx
-
论我国私营企业员工激励机制.docx
-
人教版五年级品德与社会上册全册教案.docx
-
开学啦国旗下讲话稿三分钟.docx
-
露天采矿学复习题.docx
-
六年级英语教师年度考核个人总结.docx
-
某路站综合体项PC吊装施工方案.docx
-
人教版九年级历史上册期末考试试题一套.docx
-
隆昌妇幼保健院.docx
-
芦二矿抽采达标中长期规划.docx
-
看拼音写词语.docx
-
模拟磁盘调度算法系统的设计毕业设计.docx
-
每周一条名言警句或一首诗词.docx
-
棉花膜下滴灌示范工程设计总结报告.docx
-
九年级化学教案第十单元酸和碱教案新人教版.docx
-
宁波市水资源公报.docx
-
农业实用技术培训工作意见与农业局上半年工作总结范例两篇汇编.docx
-
平行线的判定.docx
-
内部会计管理制度11成本核算制度.docx
-
盘扣式脚手架支撑方案.docx
-
旅游规划模板.docx
-
煤矿大本大专毕业设计大采高综采工作面作业规程.docx
-
美学选择题整理课件资料.docx
-
名家论腹泻慢性肠炎.docx
-
宁夏银川市第一中学学年高一上学期期中考试地理试题解析解析版.docx
-
年产吨精密纤维纸项目建设建议书.docx
-
农技推广中心工作总结.docx
-
彭宇案的法逻辑批判.docx
-
宁夏仕奇房产网发布份房地产交易情况.docx
-
项目推荐书智能温控节能系统.docx
-
区县节日期间加强消防安全讲话稿与区发改委领导班子述职述廉报告汇编.docx
-
新标准大学英语综合教程4课后习题答案课文讲解翻译Word下载.docx
-
小学二年级数学下册练习题文档格式.docx
-
烟道及导流板防磨施工方案Word文件下载.docx
-
重庆公共租赁住房管理暂行办法Word文档格式.docx
-
桥门式起重机检验方法和对比探究参考文本Word下载.docx
-
白洋淀纪事题目Word格式.docx
-
复合式中墙连拱隧道施工方案优秀Word文件下载.docx
-
高中语文第二单元测评新人教版必修3Word文档格式.docx
-
《SMT技术工艺流程及教学》课程课件Word文档下载推荐.docx
-
成都市甲级写字楼调研分析Word文件下载.docx
-
研究生招生学科专业代码册Word文档下载推荐.docx
-
专题26 光电综合计算中考物理34个典型专题突破原卷版Word文件下载.docx
-
生活中的经济学题库文档格式.docx
-
一个乡下来的小伙子去应聘城里文档格式.docx
-
四年级渔夫阅读理解精选带完整答案Word文档格式.docx
-
最新浙教版八年级上册科学知识点汇总最新版超实用Word文件下载.docx
-
新加坡签证担保书docWord文件下载.docx
-
山东省泰安市中考政治真题及答案五四制Word文件下载.docx
-
重阳节老人代表发言稿Word下载.docx
